The Utility of Routine Clinical 12-lead ECG in Assessing Eligibility for Subcutaneous Implantable Cardioverter Defibrillator
Abstract
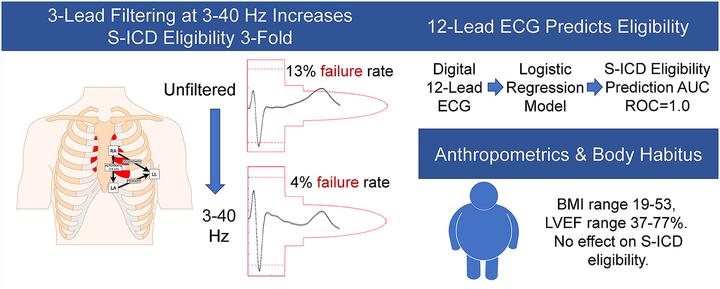
Introduction: The subcutaneous implantable cardioverter-defibrillator (S-ICD) is a lifesaving device. Recording of a specialized 3-lead electrocardiogram (ECG) is required for S-ICD eligibility assessment. The goals of this study were: (1) evaluate the effect of ECG filtering on S-ICD eligibility, and (2) simplify S-ICD eligibility assessment by development of an S-ICD ineligibility prediction tool, which utilizes the widely available routine 12-lead ECG.
Methods and Results: Prospective cross-sectional study participants [n=68; 54% male; 94% white, with wide ranges of age (18-81 y), body mass index (19-53), QRS duration (66-150 ms), and left ventricular ejection fraction (37-77 %)] underwent 12-lead supine, 3-lead supine and standing ECG recording. All 3-lead ECG recordings were assessed using the standard S-ICD pre-implantation ECG morphology screening. Backward, stepwise, logistic regression was used to build a model for 12-lead prediction of S-ICD eligibility. Select electrocardiogram waves and complexes: QRS, R-, S-, and T- amplitudes on all 12 leads, averaged QT interval, QRS duration, and R/T ratio in the lead with the largest T wave (R/Tmax) were included as predictors. The effect of ECG filtering on ECG morphology was evaluated. A total of 9 participants (13%) failed S-ICD screening prior to filtering. Filtering at 3-40 Hertz, similar to the S-ICD default, reduced S-ICD ineligibility to 4%. A regression model that included RII, SII-aVL, TI, II, aVL, aVF, V3-V6, and R/Tmax perfectly predicted S-ICD eligibility, with an Area Under the Receiver Operating Characteristic Curve of 1.0.
Conclusion: Routine clinical 12-lead ECG can be used to predict S-ICD eligibility. ECG filtering may improve S-ICD eligibility.